
The Biggest Fraud Ever, Part 1: The Hocus "Science" Behind Lockdowns Tyler Durden Wed, 07/29/2020 - 23:45
Authored by Barry Norris via Argonaut Capital,
Fraud (from 14th century Latin) n – deceit, trickery, intentional perversion of truth in order to induce another to part with something of value or to surrender legal rights: and art of deceiving or misrepresenting; imposter, cheat, one who is not who that person pretends to be: something that is not what it appears to be
Hoax (probable contraction of hocus, circa 1796) n - an act intended to trick or dupe: something accepted or established by fraud or fabrication; v – to trick into believing or accepting as genuine something false and often preposterous
Swindle (from Old English, coined circa 1782, “to vanish”) v – to take money or property by fraud or deceit.
- “Great Hoaxes, Swindles, Scandals, Cons, Stings and Scams” Joyce Madison, 1992
Frauds often have powerful counter-narratives.
When Wirecard went straight from a DAX-30 €12bn capitalisation to insolvency in June, we wondered not only why it had taken so long for the auditor to seek confirmation of cash balances but why so many investors had been hoodwinked for so long by its empty claims to have been a legitimate player at the epicentre of the digital payments industry. We had also long been inclined to believe that $4bn FTSE-100 member NMC Healthcare’s management had been siphoning off shareholders’ assets (and that the same was true of its smaller sister “fintech” company Finablr), but were bemused to see continued institutional demand for insider share placings and belief in faked takeover rumours, right up until the declared insolvency in March.
Whilst we think there is plentiful potential for further stock-market flops it is time to consider whether these serious corporate failings have now been dwarfed by the unnecessary damage caused by the “science” behind lockdown and the current parallel focus on a vaccine as the sole long-term COVID solution.

Part 1 – The hocus “science” behind lockdown
When lockdown was imposed, we were told we were facing a second Spanish flu pandemic (thought to have killed up to 50 million people); that hospitals would be overrun and there would be 500,000 deaths in the UK alone. This was a powerful and emotive narrative, but it was never true. Governments and an obedient media focused exclusively on Imperial College’s now discredited doomsday scenario built on a hypothetical, badly coded model5, ignoring its author’s history of failed doomsday predictions and the different views of other scientists.
Alternative evidence-based (i.e. theories based on facts) population samples already existed: the most prominent being the Diamond Princess Cruise Ship; which at the end of February accounted for over half of all confirmed infections outside of China. “Cruise ships are like an ideal experiment of a closed population”, according to Stamford Professor of Medicine John Ioannidis. “You know exactly who is there and at risk and you can measure everyone” .
Quarantined for over a month after a virus outbreak, the entire cruise ship ‘closed population’ of 3,711 passengers and crew, with an average age of 58, were repeatedly tested. There were 705 cases (19% total infection rate) and six deaths (a Case Fatality Rate of just 1%) by the end of March (eventually 14 in total). This compared to 116 deaths that would have been predicted by the Imperial model).
Over half of the cruise ship cases were asymptomatic, at a time when the official “science” behind the lockdown, Prof. Neil Ferguson (UK), dismissed the lack of any evidence for a high proportion of cases so mild that they had no symptoms and Dr Anthony Fauci (US) had written in the New England Journal of Medicine that in the event of a high proportion of asymptomatic cases, the COVID mortality rate would ultimately be “akin to a severe seasonal influenza” (a statement which he now at least seems to have clearly forgotten in his enthusiasm for a vaccine solution).
The cruise ship deaths were exclusively amongst an over 70’s age cohort. Although the Diamond Princess sample size was small it remains the earliest and most accurate predictor of mortality, infection and asymptomatic cases. Extrapolating this data to the wider, younger population would logically lead to downward revision on the mortality risk and upwards revisions to the level of asymptomatic cases. COVID outbreaks aboard naval ships with younger populations confirmed this: only 1 death and 3 hospitalised cases out of 1,156 infections on the USS Theodore Roosevelt; zero deaths out of 1,046 confirmed cases on the Charles de Gaulle. Even in ships which could not carry out effective social distancing the virus mortality rate, whilst a serious public health risk, was certainly not the “Spanish flu”.
As more testing was carried out across population samples (and not just on the patients hospitalised) studies came to the same conclusion: the rate of infection was higher than thought with more harmless cases and therefore the ultimate mortality risk was much lower than originally claimed. Despite this empirical evidence and the contrarian opinions of other expert epidemiologists which have since proven to be much more accurate, the Imperial College virus narrative of “the worst pandemic in 100 years”(Fig. 1) did not change: governments, the media and the official “science” doubled down on the “dialogue of doom”. Ferguson then broke his own lockdown in a tryst with his married lover and justified it by claiming he had antibody immunity (which given what we now know about decaying antibodies may not have been correct).
Fig 1. COVID-19 mortality in perspective

The population mortality risk of the virus was initially estimated at 3.8% by the WHO which had arrived at this number simply by dividing the number of Chinese deaths by the number of confirmed cases, ignoring the fact that only a small proportion of likely infected people had actually been tested; that asymptomatic cases were likely to be significantly underrepresented in testing and that the more serious cases were likely highly correlated to serious symptoms. This basic statistical error of simply dividing deaths by reported infections not only exaggerated the severity of the risk but led directly to policy error on hospital capacity and care home deaths.
Media reporting also intentionally failed to acknowledge that mortality risk was highly skewed to age (median mortality age of 8229) in order to scare the entire population into observing lockdown with falsely exaggerated media reports of young and healthy people dying from the virus. Mortality risk amongst the elderly was skewed to those with existing health issues (the presence of comorbidities) with Italy reporting that 96% of virus fatalities also suffered from other illnesses, but this did not fit the desired narrative. Whereas the Spanish flu in 1918 had disproportionately killed the young and healthy – meaning that each death lost more years before predicted average mortality – COVID deaths on average occurred at or beyond average life expectancy, which was always consistent with a normal mortality risk curve, and seasonal non-pandemic coronavirus.
Fig 2. UK COVID deaths by age and presence of comorbidities

It was also originally wrongly assumed that the hospitalisation rate of the virus based on Chinese data could be as high as 20% (ten times higher than influenza) hence the focus on ensuring that hospital intensive care units were not over-burdened. The overall hospitalisation rate in New York City is reported as 25% based on reported cases but this figure comes down to just 1.5% based on predicted infections based on antibody tests (55,000 hospitalisations out of an estimated 2.7 million infected). New intensive care hospital capacity was built (but never used), non-COVID treatment cancelled with likely consequences for excess mortality far more disastrous than COVID and infected hospital patients moved to care homes with disastrous consequences. This policy mistake occurred primarily as a result of panic and the statistical error of drastically over-estimating the mortality and hospitalisation rate through under-estimation of asymptomatic cases. Whilst widespread testing was not necessarily available, public health authorities could have studied the facts of the COVID outbreaks on the boats rather than rely on Ferguson’s “rubbish-in-rubbish-out” model.
Deaths in care homes are now estimated to have accounted for half of all COVID related mortality (Fig. 3). Similar failures to isolate COVID patients in hospitals are thought to have been responsible for up to 20% of all infections in the UK and 40% in Wuhan. All of this could have been mitigated by isolation of those infected and those treating the infected which need not have been dependent on a general lockdown of the entire population. When this point was put to Ferguson he responded by dismissing the specific isolation of the “old and vulnerable” as “wishful thinking” simply because it had previously never been done, as if putting the wider economy into lockdown was simpler, with precedent of success and no unintended negative consequences. The accusation remains that lockdown was at best a sledgehammer to crack a nut: mitigating nosocomial infections never required lockdown.
Fig 3. Care Home deaths by country

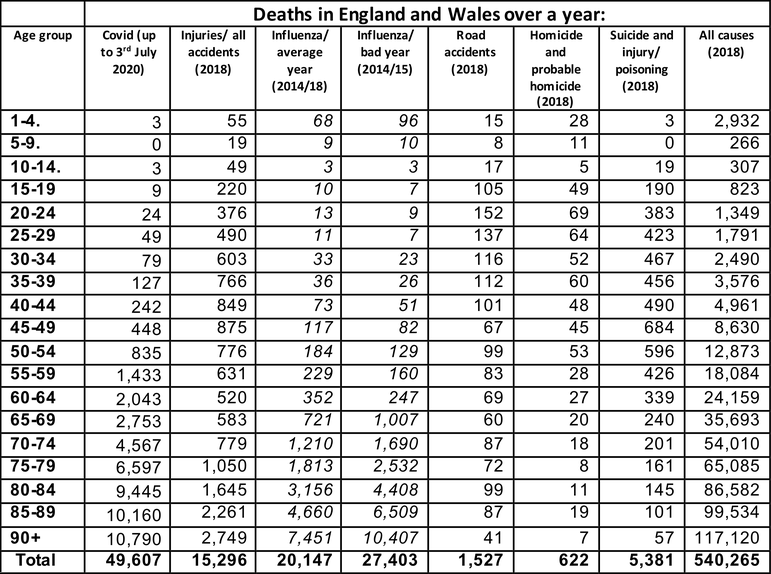
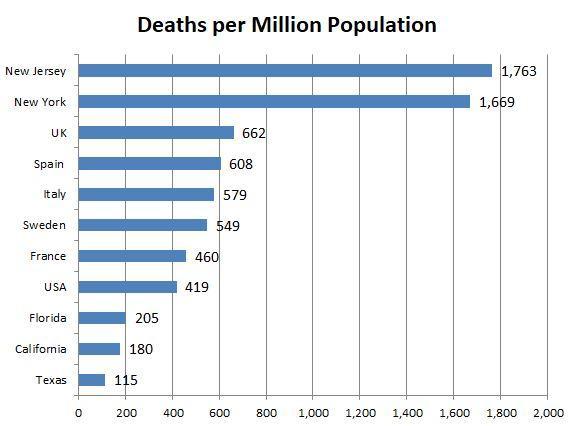
New York State Governor Andrew Cuomo (who was to preside over the worst mortality rate (Fig. 6) of any US state) summed up the emotional policy response when announcing a strict lockdown in March with the justification that “if everything we do saves just one life, I’ll be happy”. There was no acknowledgment that lives were at risk from other causes of death due to lack of treatment and that this risk could be magnified by the lockdown. Did Cuomo realise that there were on average 150,000 daily deaths globally of which half were accounted for by cardiovascular diseases and cancer, which could also be mitigated if targeted by public policy with the same urgency as COVID? The 650,000 reported COVID deaths worldwide are rarely put into the perspective of 33.4 million deaths globally so far this year. Moreover, it was becoming clear that the mortality risk for most of the population from COVID, whilst not zero, was statistically lower or comparable to an average influenza season, road accidents or suicide (Fig. 4) But perhaps because COVID was a new, unknown cause of death, proportionality got lost: the mission was not to just “flatten” the infection curve but to be seen trying to prevent ALL COVID deaths.
Fig 4. UK COVID deaths by age vs. other causes of mortality
Nevertheless, Imperial College continued to argue that lockdowns had saved millions of lives (based solely on reality being radically different from their doomsday model). By now it had become clear that there was a significant element of society that enjoyed authoritarianism for its own sake and whatever the evidence to the contrary, were now inclined to believe that the withdrawal of civil liberties and economic destruction in the name of protection from COVID (but not any other source of mortality risk) was always justified and its proportionality or unintended consequences never questioned. By now Dr Fauci – who had avoided Ferguson’s personal disgrace – had become a household name in the US. He continually warned about the dangers of re-opening too quickly, but when challenged about “trade-offs” for the economy or other non-COVID health factors, of what he regarded as an “inconvenient” situation resulting from lockdown, it was clear that his advice was solely one-dimensional:
“I’m a scientist, a physician, and a public health official. I give advice, according to the best scientific evidence. There are a number of other people who come into that and give advice that are more related to the things that you spoke about, the need to get the country back open again, and economically. I don’t give advice about economic things. I don’t give advice about anything other than public health.”
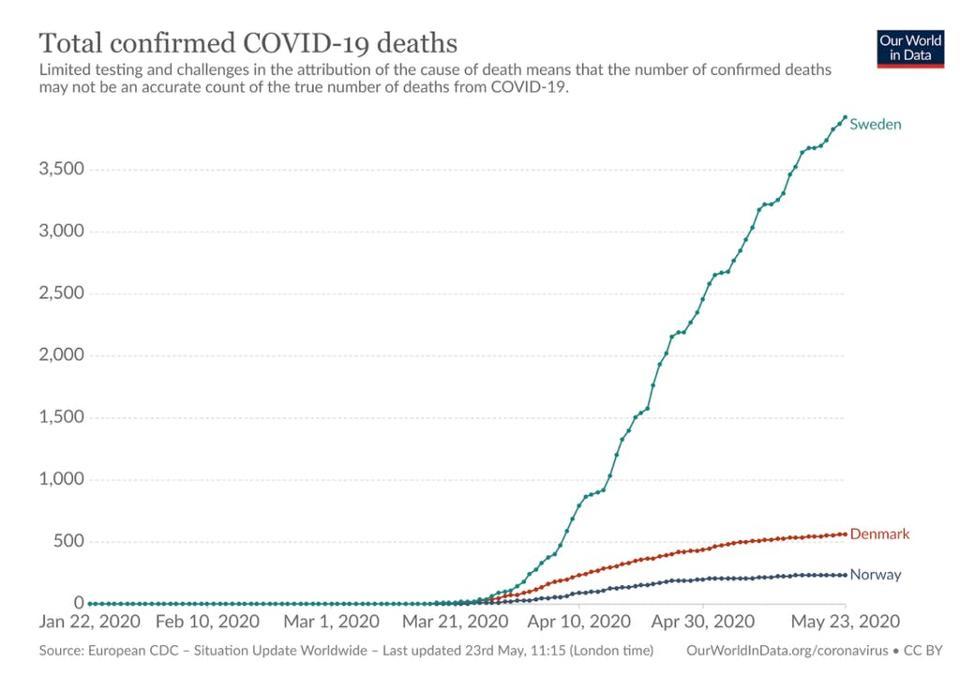
The Swedish government had been unique in recognising the trade-offs between COVID public health and other factors a rational, non-panicked, responsible government might consider and had chosen to implement social distancing but not lockdown. It therefore became a dangerous experiment which could not be reported as succeeding whatever the objective truth. Whilst even Ferguson begrudgingly accepted that Swedish mortality was a fraction (6%) of his prediction of 96,000 deaths by June (he claimed because Sweden had in his view done a kind of phantom lockdown without telling the outside world), other lockdown fanatics began distorting statistics by highlighting Swedish infections (Fig. 5) on a cumulative basis or comparing to other Scandinavian countries with different situations; as Sweden had a higher initial infection rate in a larger and more densely populated country, so the outcome could never be compared as a measure of success).
Fig 5. Media reporting of Swedish COVID deaths
More outrageously, when the leading Swedish epidemiologist admitted to “mistakes” in the management of care homes (which accounted for 75% of Sweden’s 5,500 deaths with an average age of 86) this was bizarrely and widely reported by supposedly reputable media outlets as an admission of failure of the overall policy.
To put the Swedish “failure” to lockdown into further perspective, there are around 2,000 -3,000 deaths (from a 10 million population) in Sweden annually in a normal flu season. Nevertheless, for lockdown to have been justified the Swedish mortality rate should have been anomalous – it was not (Fig. 6). The control group and the experimental group produced similar mortality outcomes.
Fig 6. The Swedish Anomaly?
Not only did Ferguson’s lockdown model over-estimate Sweden’s deaths by a factor of 20 but Sweden also produced the same mortality and infection curve as the UK (and most other similarly urbanised European countries) and a significantly flatter infection and mortality curve than New York (Fig. 7) even comparing Stockholm with New York State (Fig. 8) (with Stockholm having over 2.5x more population density that NY State).
Fig 7. Sweden’s curve flattens without lockdown
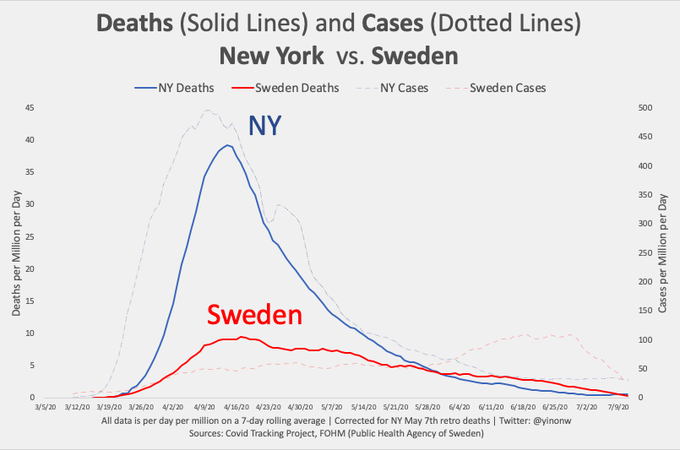
Fig 8. Stockholm’s curve compared to New York State
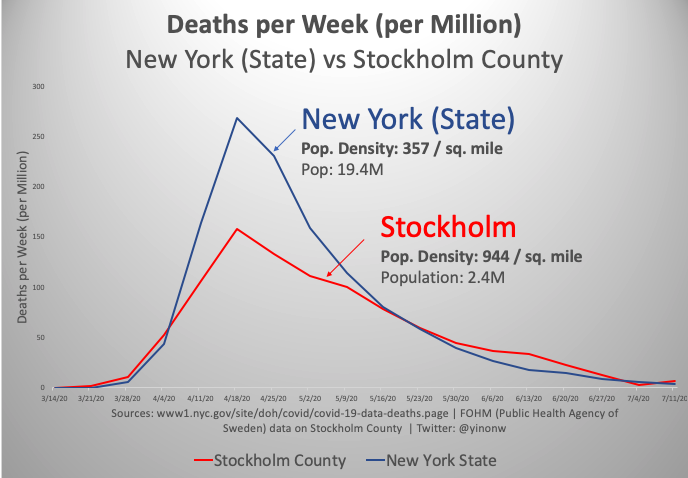
The “shape of the curve” was unaltered by differing lockdown policy. At best the efficacy of lockdown was unproven but then there were also the unintended consequences and trade-offs that Fauci might not consider but responsible governments might . If it were a drug trial, lockdown would have been pronounced a failure and the experiment stopped.
Subsequently, a range of scientific studies have now shown that government actions had no statistically significant reductions in the number of critical cases or overall mortality. Given the economic catastrophe, social breakdown and neglect of non-COVID healthcare this was a devastating policy error. When by July (Fig. 9) the virus had all but disappeared from Sweden there was no positive acknowledgement from other governments which had implemented lockdown and no reporting from their lapdogs in the media.
Fig 9. The virus disappears from Sweden to be acknowledged by…complete silence
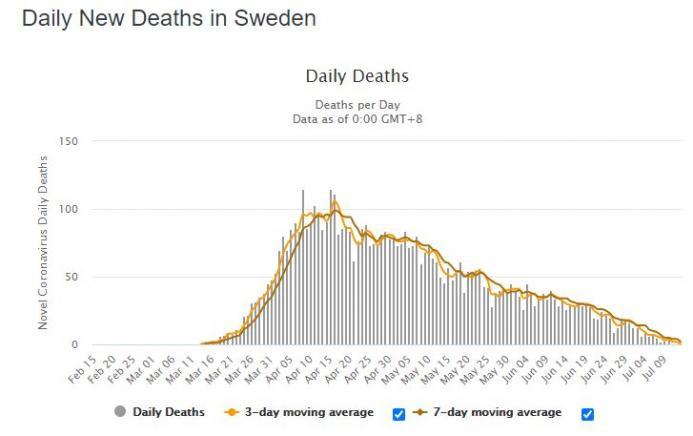
Just silence.
* * *
Fully hyper-linked reference list available here
Part 2 (of 2) - "The Vaccine Swindle" will be released tomorrow
https://ift.tt/30cVN2l
from ZeroHedge News https://ift.tt/30cVN2l
via IFTTT



0 comments
Post a Comment