
The Biggest Fraud Ever, Part 2: The Vaccine Swindle Tyler Durden Fri, 07/31/2020 - 00:00
Authored by Barry Norris via Argonaut Capital,
It was originally assumed that only those who had previously been infected by the virus and developed an antibody response had any immunity, hence the initial focus on testing for the presence of these antibodies as well as infection. However, studies of antibodies in formerly infected patients demonstrated accuracy issues which subsequently could be explained instead by the antibodies’ rapid decay in recovering patients. The often disappointingly low levels of antibodies in population samples is often used as evidence that herd immunity is not a realistic goal without a vaccine.
This is not correct.

At the end of May there was a significant breakthrough in understanding of COVID antibodies which was not widely reported: a Swiss study from Zurich led by Professor Onur Boyman demonstrated that a large proportion of the population had a natural immunity through existing antibodies on the mucous membrane (IgA) or cellular immunity (T cells), likely to have been acquired through previous exposure to coronaviruses such as influenza or the common cold (the absence of exposure to previous coronavirus is now thought to explain the opposite effect in 1918).
The study found that that the presence of (IgG and IgM) antibodies generated on infection which tests had previously focused on, were NOT in fact required to defeat the virus and that existing (IgA and T cell) antibodies that gave a natural immunity. Moreover, the population with this natural immunity was demonstrated to be five times greater than those with the IgG and IgM antibodies on which tests had hitherto focused. If this could be substantiated, then the population already exposed to COVID would also be five times greater than previously assumed. In other words, if a population sample showed 10% had IgG and IgM antibodies (which might be subject to decay) then it was likely that at least half of the population had already been exposed to COVID.
It followed that antibody studies that measured only IgG and IgM that were now predicting population-based mortality risk of 0.1% to 0.5% (lower than the 1% in the elderly population aboard the Diamond Princess) could be even further reduced by a factor of five to 0.02% to 0.1% and the level of symptomatic exposure from 20% to below 5% (consistent with the flu season ironically predicted by Fauci in March). Not only would this mean a further similar reduction in the estimated true mortality rate but it meant that there were far fewer people in the population who had never had exposure to the virus, so a far lower number who could potentially catch the virus in the future.
In short, the infamous herd immunity was much closer than previously realised.
Fig 7. Sweden’s curve flattens without lockdown
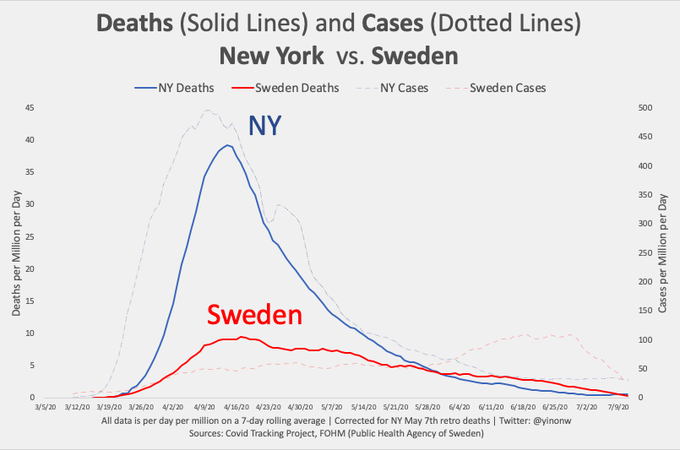
This explained why, by July, the virus had all but disappeared in populations like Sweden, New York (Fig. 7) and Wuhan (which reportedly tested its entire population of 11 million and found only 300 cases, all of which were asymptomatic) which were significantly affected by a “first wave”: if the ratio of those with IgA and T cell antibodies to IgG and IgM antibodies across population was confirmed at a factor of five then if 20% of the population had traditional IgG and IgM antibodies (such as New York with 21% and London with 17%) then the virus died out because there was simply no one left for it to infect. It followed that the virus could only survive in population samples where testing showed the presence of IgG and IgM antibodies was below 20% (and allowing for their decay probably well below).
Nobel Prize winning biological scientist Michael Levitt had already come to the same conclusion based on a different approach: he predicted that the virus would “burn out” when it had infected 15-20% of the population though based on a pattern predicted by the “Gompertz curve” which indicated that the number of deaths after the peak is roughly double those from before resulting in Levitt accurately predicting the number of Chinese and Swedish deaths, months in advance. Levitt has recently bravely predicted that US COVID will “be done in 4 weeks [25 Aug] with a total reported death below 170,000”, compared to 149,000 today.
Boyman’s theory on “IgA and T Cell immunity” explained the accuracy of Levitt’s “Gompertz curve” predictions and this was now being backed up by the empirical evidence which showed that the populations which were hit hardest with high initial rates of infection and mortality, were the ones where the virus had almost disappeared.
Almost none of this was reported by a media which choose instead to attach the misnomer “second wave” to outbreaks of COVID infection in populations which had not yet experienced any meaningful “first wave”: the Sunbelt states in the US, Australia, Hong Kong, Japan. The irony was that the vulnerability of populations which had not yet seen meaningful infection outbreaks and therefore the fallacy of lockdown had already been predicted by Levitt and Giesecke. It was also logical that population groups where IgG and IgM antibodies were still significantly below 20% would continue to see infections.
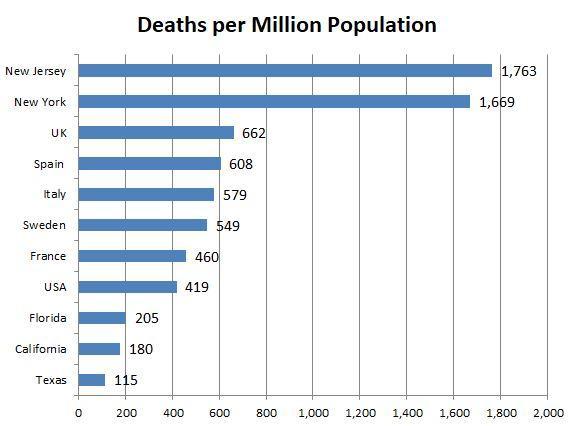
COVID had become particularly political in the US. Despite the anomalously poor Democratic New York and New Jersey records on COVID mortality (Fig. 6), there was hysterical reporting of rising infections, from very low levels, across Republican states (Florida, Texas and Arizona) which had largely avoided severe lockdown restrictions.
Fig 6. The Swedish Anomaly?
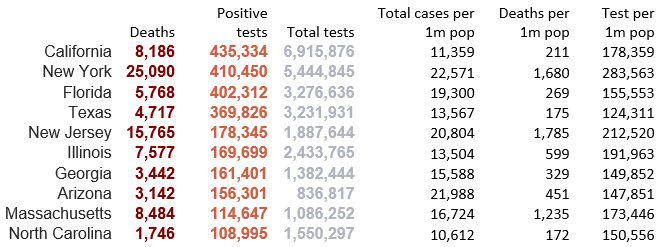
The same rising trend could also be observed in Democratic California which had been subject to lockdown but was largely avoided in Republican Georgia which was notable in its lockdown defiance (Fig. 10). The suspicion remains that infections will continue to rise irrespective of lockdown until populations have reached herd immunity at which point the virus will largely disappear. The anomalously high death rates of New York and New Jersey could be explained by their being affected at a much earlier stage before better understanding of hospital treatment and curtailment of infection in care homes . As hard as the lockdown fanatics looked, there was no correlation of infections or mortality to lockdown policy.
Fig 10. Analysis of US states and coronavirus
It was a clear misnomer to label rising reported infections in the US sun belt as a “second wave” if these states had never suffered from a “first wave” and rises in infection rate were a predominantly caused by more widespread testing of mostly younger people testing positive for COVID with no symptoms. It must also be borne in mind that “case numbers” are simply people reported as testing positive for COVID, almost entirely without symptoms, with no commensurate leap in hospitalisations or mortality, which has been conveniently ignored as not fitting the narrative. This also led to doubts about whether test results were being accurately reported with reports that some clinics were not reporting negative test results and others reporting cases as simply “probable infections” with individuals having some of the symptoms of COVID but not having been tested.
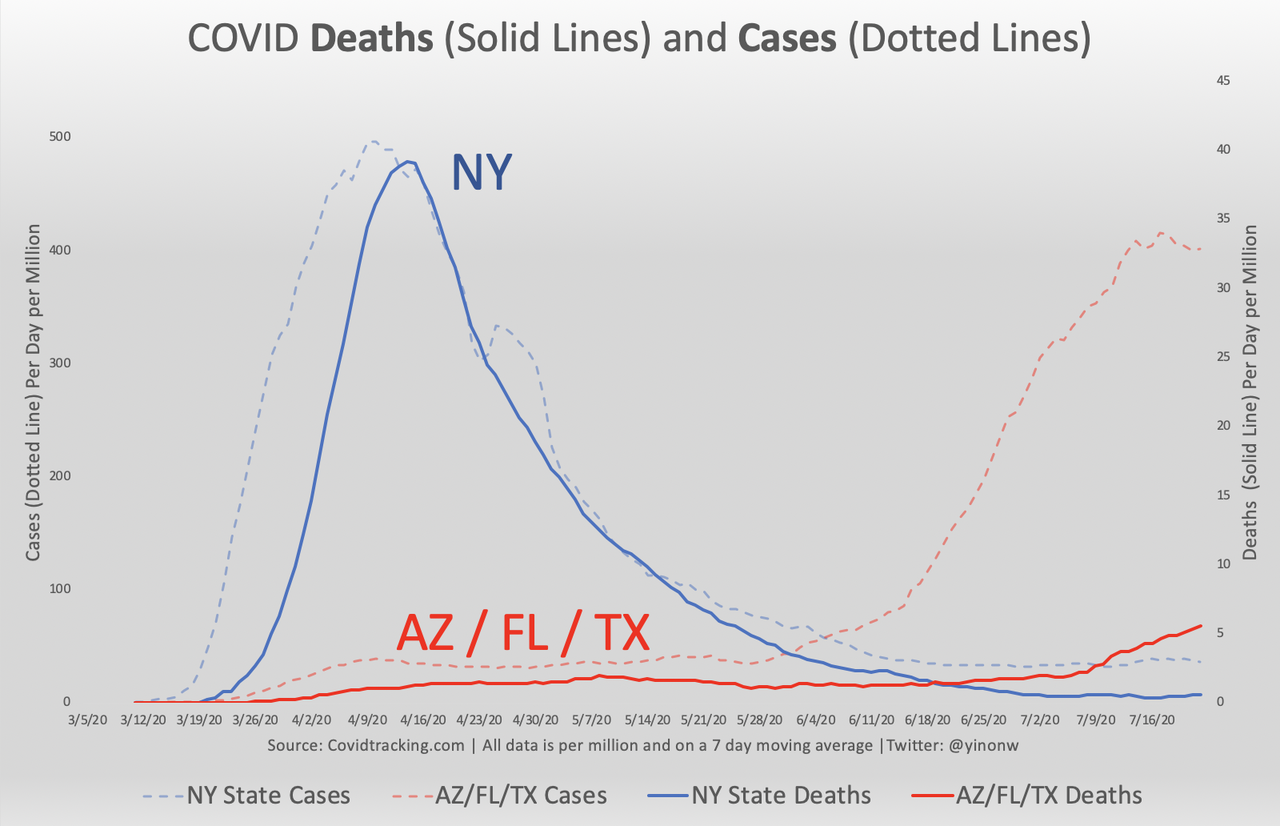
We must also note that although infections in Arizona, Florida and Texas have seen a similar spike to that witnessed in New York, the mortality remains mercifully lower to a substantial degree (90%) (Fig. 11) which can only be explained by rising testing of a younger population median (since the hospitalisation rate is also lower), better hospital treatment and an improved care home policy (at which New York and New Jersey were anomalously poor). Although we should clearly expect mortality rates to rise in the sun-belt states from very low levels, it is likely that overall mortality remains well below New York levels and beings to taper off when infections begin to peak (which according to Levitt is still a few weeks away).
Fig 11. COVID “first wave” infection curve of AZ/FL/TX similar to New York but mortality 90% below
We should also expect the mortality rate to reduce further as hospital treatment has evolved. We now know that invasive use of ventilators in fact caused COVID deaths which was particularly unfortunate given the initial scandalous news reports on their initial shortage and in the US questionable financial incentives for nursing staff to use ventilators. Doctors have also realised that the specific cause of death in many cases is pulmonary embolism, which can be treated though cheap and well-established blood-thinning medication. Several studies have also shown early intervention with the use of zinc and malaria drug hydroxychloroquine in combination has an immediate significantly reduced hospitalisation rate, of up to 80% and mortality by 50%. There is a great irony that the mortality rate could be reduced to almost zero by proven inexpensive drug combination, though this is not necessarily in the interests of the pharmaceutical industry which would prefer there to be a need for costly new drugs and vaccines.
Yet inexplicably we still hear the daily groupthink catechism that the only “long-term solution” to beating COVID is a vaccine, often without any understanding of the historic limitations of vaccines particularly in the immunisation against coronaviruses (there is still no vaccine against the common cold and vaccines against influenza are patchy in their effectiveness).
A significant obstacle to a successful vaccine is the rapid degradation of IgG and IgM COVID antibodies meaning that even a successful vaccine might not give any benefit for longer than a few weeks. As the CEO of world leading testing company Roche Diagnostics recently commented:
“What appears to happen is that people do lose antibodies over time. And that of course poses the question, will vaccines actually work if you lose antibodies”.
Reports of successful antibody responses amongst healthy adults in vaccine trials should be viewed with more scepticism. It is also almost certain that any antibody response would be more difficult in population samples with impaired immune systems that are most at risk from COVID. Even an efficacious vaccine might have to be ramped in dosage that would be intolerable to those most likely to benefit from vaccination. Leading Swiss epidemiologist Pietro Vernazza has demonstrated that the high-risk group is least likely to respond to the vaccine since their immune system is already impaired. Whilst it is possible for vaccine trials to demonstrate antibody responses, whether these will have any practical lasting benefits in reducing COVID mortality risk which are tolerable for the population group most at risk from COVID is unlikely.
Vaccines hastily developed, rushed to market without proper trials by panicked governments ready to throw money at any promising trial candidate, creates a clear moral hazard for pharmaceutical companies and a public healthcare risk which might rival the virus itself. We remain sceptical of biotech companies raising equity on tricked up trials, only never to deliver medication that has any practical application, or insiders dumping stock after supposedly promising “game changing” data, or even worse mandatory vaccination of a population on the basis of an erroneous assumption that herd immunity hasn’t already been reached, with the potential for dangerous and unnecessary side-effects in population groups who would otherwise (if they had not already been exposed to COVID) have been asymptomatic.
There is a notable discrepancy between binary expectations that a vaccine will solve COVID and the definition of success for those involved in developing a vaccine. According to Sarah Gilbert, who leads the Oxford Astrazeneca experimental vaccine:
“We need a vaccine with a high level of efficacy against disease, which also has a significant impact on virus transmission. It doesn’t need to cure you… We want a vaccine to stop people from going to hospital and dying. If you can do that, I think people will be pretty happy"
In other words, Gilbert’s definition of “success” was mitigation rather than cure, which better hospital treatment is already achieving anyway.
There is a more fundamental question of whether a vaccination program for the entire population is at all desirable, given that most of the population has a natural immunity, only a small cohort develops symptoms, an even smaller cohort at risk of hospitalisation and the best estimate of mortality risk from COVID now almost statistically insignificant. We are probably already at the stage in terms of hospital treatment whereby no one who does not already have existing comorbidities should die from COVID. If any vaccine does not stop transmission and comes with side-effects which may be dangerous (and could potentially cause a mortality risk where one was previously absent, such as the potential neurological damage caused to children from the vaccinations against “swine flu” a decade ago) it has to be asked whether the exclusive promotion of the vaccine solution by the pharmaceutical industry (and the advice of potentially compromised public health officials like Fauci) is now more likely to end up an investment swindle.
We now know that there was no credible “science” behind lockdown and whilst its imposition may have originally been motivated by the precautionary principle, the perpetuation of the “Spanish Flu” narrative has been a uniquely destructive, particularly considering the exclusion of healthcare provision for non-COVID illness, prolonged absence of child education, and the well-documented economic devastation. Although our understanding of COVID is by no means complete, we now know that its mortality risk can be best mitigated by the management of infection within the care home and hospital environment, better immediate treatment of hospitalised patients and sensible social distancing measures. None of this required lockdown. Nor does it require a vaccine.
The degree of intentionality behind the actions taken by governments, the media and the pharma industry is an unknown, but this continued perpetuation of that narrative in contrast to the empirical evidence is arguably the biggest fraud of all.
https://ift.tt/2Dj9h3y
from ZeroHedge News https://ift.tt/2Dj9h3y
via IFTTT



0 comments
Post a Comment