
Is The Coronavirus Pandemic About To Become Another Spanish Flu
Authored by Michael Every of Rabobank
COVID-19 vs The Spanish Flu
Summary
- In light of the recent outbreak in Europe, it appears a question of when –rather than whether– the COVID-19 epidemic will be declared a global pandemic
- Countermeasures such as quarantine or travel bans remain necessary to contain the virus’ spread. This will continue to cause disruption, as policy makers chase a moving target
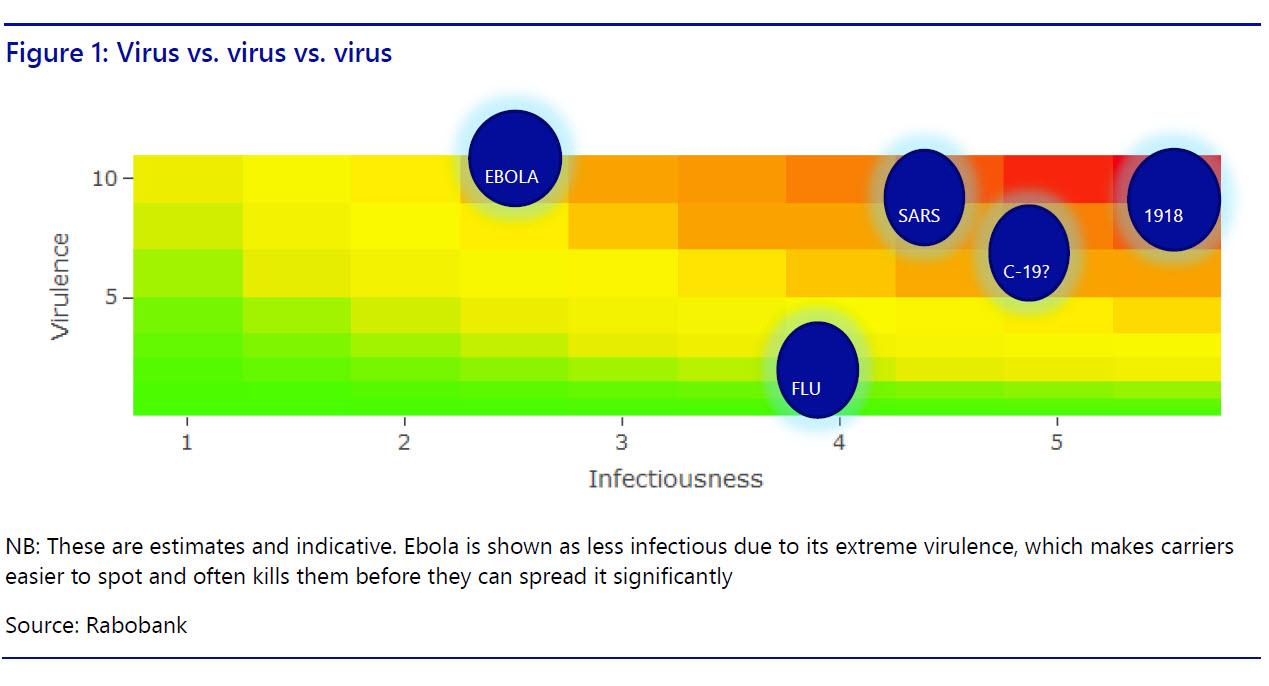
- There is an increasing interest in the 1918-19 Spanish flu, and there are indeed some similarities in terms of virulence, infectiousness, and the potential attack rate.
- Anecdotal evidence suggests a similar economic impact both despite and because of changes in society.
- The key lesson from COVID-19 is the same as with the financial sector: complex interconnected systems greatly increase underlying risks, which are multiplicative and exponential, rather than additive and linear.
Chasing a moving target
Since the middle of January, the number-one worry for businesses, policy makers and market participants has been the outbreak of a new coronavirus known as COVID-19. In an effort to gauge its potential impact, analysts initially resorted to comparisons with the outbreak of SARS and MERS, two previous diseases resulting from coronaviruses. But we are now already way past this. It appears a question of when –rather than whether– this epidemic will be declared a global pandemic.
This is why there has been an increase in interest in previous pandemics. In particular, we have noticed a lot of comparisons with the ‘Spanish flu’, which originated in the final year of the First World War, spread rapidly, and resulted in an estimated 50-100 million deaths worldwide. So far, COVID-19 has led to more than 80,000 illnesses and 2,700 deaths, predominantly in China’s Hubei province, but more recently also in places such as South Korea, Iran, and Italy.
At the same time, we have also heard plenty of comparisons with another viral epidemic: the seasonal flu. In the US alone, the Centers for Disease Control and Prevention (CDC) estimates that so far this season there have been at least 26 million flu illnesses, 250,000 hospitalizations and 14,000 deaths. It is then argued that COVID-19 isn’t much of a big deal compared with seasonal flu, and that ‘business as usual’-conditions should return as soon as possible.
This is too complacent. Virologists have studied seasonal flu for decades. Despite the high number of illnesses, we generally have a good idea on what to expect. As the Northern Hemisphere moves towards spring, it is certain that flu cases will go down. In contrast, very little is known about COVID-19. Its basic reproduction number is also unknown, but the explosive rise in cases signal that it’s significantly higher than 1. Therefore, countermeasures such as quarantine or travel bans remain necessary to contain the virus’ spread.
The philosopher Søren Kierkegaard once wrote that “life can only be understood backwards, but it must be lived forwards”. Indeed, COVID-19 appears to be a wild card in terms of how far it will spread, how many deaths it will cause, and how severe the demand and supply shock is going to be. Let’s find out whether the Spanish flu could provide us with some pointers.
La gripe Española
The Spanish flu was a strain of avian influenza. Starting in late 1917, the virus spread across Europe, North America and Asia. Initially, it resembled seasonal flu, and those most at risk were the sick and the elderly. But around August 1918, the virus mutated to a much deadlier form, and deaths peaked between September and November 1918, eventually culminating in an estimated 500 million infections and 50-100 million fatalities. The Spanish flu is therefore the deadliest pandemic in human history, claiming many more lives than the First World War itself.
Whereas infectious diseases prior to the Spanish flu had mostly spread along trade routes (the 14th century Black Death is a good example of how intensified contact along dense networks increases a disease’s potential), the global context of the First World War appeared to enable the great spread of this flu. There was a lot of movement and interaction between people –with and without guns– and transmission was facilitated by extremely poor sanitary and health conditions.
The pandemic occurred in three waves with different characteristics. The first originated in early March 1918, and was a relatively mild one. The second wave was extremely deadly and came in the autumn of 1918. The third and final wave took place in the winter of 1919. Virologists have proposed several mechanisms to explain why this flu came in waves, including viral evolution (e.g. mutations), environmental changes (e.g. the weather) and behavioral changes in response to the pandemic (e.g. containment efforts), but there appears no real consensus of the interactions of these factors. This is partially due to data limitations and a lack of expertise at that time.
It has also been hypothesized that the unique circumstances of the First World War altered the virus’s natural selection process. Typically, the dangerous strains make their hosts very sick, who then recognize their symptoms relatively easily and move either into quarantine or pass away rapidly. These strains tend to die out relatively quickly – even if it is with their hosts, in the case of Ebola, for example. Milder strains, on the other hand, make people only mildly ill. Their hosts will have a stronger tendency to remain active in public life, and to expose others with these milder strains. One benefit of this is that it (partially) improves immunity to the more aggressive strains. In the First World War, however, very sick soldiers were sent on very crowded trains to even more overcrowded field hospitals, while the mildly ill remained at the front. This eventually helped spread deadlier strains in the second half of 1918, wreaking havoc in those parts of the world were the milder strains hadn’t presented themselves yet.
Comparisons with COVID-19
A rather similar epidemic?
As it stands now, COVID-19 seems to be a virus with relatively modest virulence: the case fatality rate being estimated to be around 2%, much lower than SARS or MERS. However, it has relatively high infectiousness. with the initial estimates of R0 –the basic reproduction number– are around 2.5. Simply put, this means that each case can generate 2.5 other cases. This may change over time, as people adjust their behavior, yet the relatively long incubation period for COVID-19 (perhaps up to 27 days) ensures that people can carry and transmit the virus without showing any symptoms.
The Spanish flu had a case-fatality rate of more than 2.5%, although estimates vary, and a reproduction number in the range of 2.0–3.0 in cities (which is what we should look at now, given the population shift from rural areas to urban areas). In other words, if countermeasures are as ineffective in containing the virus as they were in 1918-1919, when they were arguably non-existent, it could be argued that the current virus has a potential attack rate of 60-80%. We can therefore learn from the Spanish flu that as long as this virus remains transmissible but relatively mild, it has the potential to spread rapidly around the world. This pessimistic theoretical approach has been backed up by the Harvard University epidemiologist Marc Lipsitch.
What’s in a name? The rose still stinks regardless
The origins of the Spanish flu remain shrouded in mystery, even though it is generally accepted that there was very little Spanish about it. Instead, Spain was a neutral country in the war and the freedom of its press was greater than in the warring nations. As a consequence, there were lots of reports about the virus’ devastating effects in Spain, while in most other European countries any information that was likely to impact morale or indicate weakness was strongly censored.
We can draw a parallel here. Even though China has now taken extreme precautionary measures to limit the spread of COVID-19, they were rather late in their response. The authorities have also acknowledged this recently. But as the Chinese government continues to control the flow of information it is likely that a wide distrust in the officially published data on cases and fatalities will remain. The same holds true in Iran, for example, while many other countries, even the US, are not really testing their populations to any real extent: no tests means no cases – but it does not mean no virus is present.
But does that still matter at this point? While the lack of good and timely information potentially contributed to the initial spread of the virus, the genie is now out of the bottle. Moreover, whether the virus is or is not present does not seem to be altering the pattern of public behavior much. With full transparency of the risks people generally go into panic-buying mode and then into a voluntary lockdown almost as aggressively as they do under a state-imposed quarantine: for example, Chinese restaurants are deserted, even in areas of countries with no reported virus links.
The public reaction in some countries to date already seems to echo the panic seen in 1918-19.
Not W-shaped, but J-shaped
The curve of influenza deaths by age has historically been U-shaped, but the Spanish flu had a W-shaped curve. It was extremely deadly for those in the 19-40 age cohort, who are usually least vulnerable to viruses. This is in stark contrast to the mortality rates for COVID-19, which seems to have the worst impact on those aged over 65 and/or with co-morbidity factors such as diabetes, lung and/or heart conditions. This would then be a J-shaped curve.
The figures below are based on a study that examined data from 72,314 patients and was carried out by a group of experts at the Chinese Center for Disease Control and Prevention. This would seem to argue for COVID-19 to present a much less significant threat to the global economy than its predecessor a century ago. However, we would argue that this overlooks some mitigating factors.
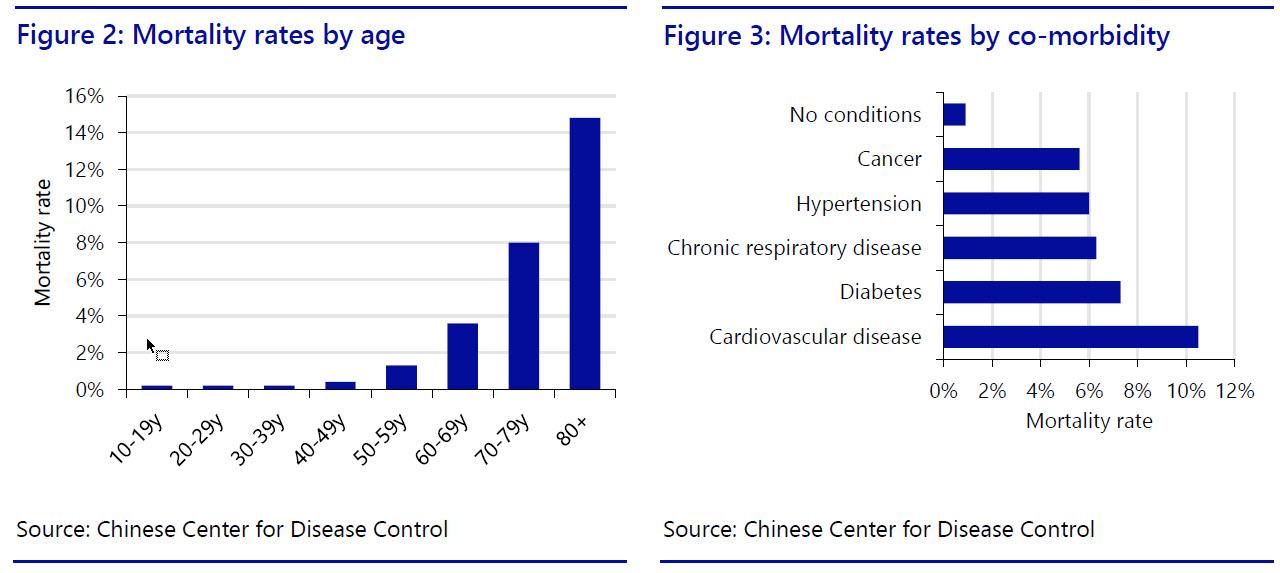
Notably, the population profile of developed countries today, where the most economic damage could be done, skews significantly higher than it did back in 1918-19 in its own J-shape. This means that while younger people have less to worry about with COVID-19 than with Spanish flu, there are more of those who are potentially most vulnerable to the current virus. For example, the average life expectancy in the US was around 56 years in 1919, well below the 65+ band where COVID-19 seems to do the most damage today. Moreover, more than 16% of the US is aged over 65, and so most at risk from the virus, and that rises to 27% in Japan, 23% in Italy, 22% in Portugal, 21% in Germany, and 20% in France.
Second, although healthcare today is vastly superior to that of the early 20th century in almost all locations, which is a huge comfort, it is also much more expensive than the relatively simple treatments available in 1918-19, and hence more rationed. While a fully-equipped ICU may ensure a better and faster recovery from a virus, how many ICU beds would be available to patients if the elderly demographic were to fall victim to COVID-19 en masse in each country? They would be overwhelmed, as we already see from normal seasonal flu epidemics in the UK, and currently in China, a country which despite aging rapidly still only has around 12% of its citizens aged over 65. Meanwhile, in emerging economies with a much younger demographic, which is a positive, the public healthcare systems are generally far weaker and less prepared, meaning that the virus can again potentially still wreak havoc.
In short, COVID-19 could still potentially compare with the Spanish flu - in a worst-case scenario.
Fear and trembling, indeed
From a purely economic perspective, there isn’t a lot of data which we can use to examine the impact of the Spanish flu with any sort of precision given the absence of detailed national accounts data in most countries. Clearly, however, 1918-19 was a totally different structure for a virus to hit. Agriculture still accounted for a far larger share of GDP than today, and rural economies were still relatively more important: in those areas, the virus spread less rapidly due to lower population density.
By contrast, the bulk of today’s economy is about the urban environment and services, the former the prime environment for virus transmission. Moreover, both cities and services are hit hardest by any virus lockdown, making the modern economy arguably even more susceptible than in 1918-19 despite our advances in technology and communications. For example, a 2009 UK study found that even in a mild pandemic scenario the economic cost would be 0.5-1.0% of GDP, rising to 4.3% of GDP, and potentially even higher, in the case of a severe “high fatality” scenario. (Please see our recent special report on the potential global economic impact of the virus.)
Clearly, however, there are already some worrying parallels between Spanish flu and COVID-19. For example, this paper published by the Federal Reserve Bank of St. Louis contains some anecdotes that any person who reads today’s business news might very well recognize. We’ve picked just three:
- “Merchants in Little Rock, Arkansas say their business has declined 40%. Others estimate the decrease at 70%.”
- “The only business in Little Rock in which there has been an increase in activity is the drug store.”
- “Physicians report they are kept too busy combating the disease to report the number of their patients and have little time to devote to other matters.”
More broadly, the authors also surveyed economic research and conclude that most of the evidence indicates that the effects of the 1918-19 pandemic were short-term. Then again, there was a lot of euphoric post-war reconstruction that needed to be done in 1919 in Europe at least, which flowed through to the US economy to some extent. Today’s businesses seem to find it hard to locate profitable investment opportunities despite ultra-low rates, and a further sharp drop in global demand is all that they need.
The Fed also found that back in 1918-19 “a decrease in the supply of manufacturing workers that resulted from influenza mortalities would have had the initial effect of reducing manufacturing labor supply, increasing the marginal product of labor and capital per worker, and thus increasing real wages”. Yet another study on the impact of the 1918 pandemic on Swedish economic performance found robust evidence that “the influenza had no discernible effect on earnings” but that it instead led to “a significant increase in poverty rates” – obviously as the state played a much smaller counter-cyclical role in 1919 than it does in 2020.
In today’s economic environment, where wage growth has proved almost universally sticky to the downside, we find it very hard to believe that COVID-19 will lead to an increase in real wages – at least near term. Rather, for developed economies with ever more ‘gig’ workers and self-employed, even in developed economies, an increase in poverty appears far more likely, ceteris paribus.
In short, the 1918-19 Spanish Flu massively disrupted a global economy already shattered by the First World War (1914-18). COVID-19, while so far much less virulent in some key respects, also looks potentially able to do a huge amount of damage to a modern global economy with its own pre-existing health conditions.
‘Stating’ the obvious
However, unlike in 1918-19, the state will almost certainly step in: populations, and markets, will demand it. Fiscal spending will accelerate hugely, with little concern over deficits, just as would be the case in a war. Even traditionally-prudent Hong Kong, hard hit by both political unrest and now COVID-19, has just announced a HKD10,000 (USD1,274) fiscal transfer for each adult permanent resident to try to jump-start the economy. Yet can a virus-hit emerging market do the same? That seems highly unlikely. Indeed, some emerging markets are incapable of testing for COVID-19 and others are charging for doing so (and for treating it), which ensures the poor will try to avoid reporting any illness. As such, the virus could have a ‘home base’ to linger in and spread from.
Even in richer economies physical bottle-necks, e.g., ICU beds, would remain for a long time. No other country can build a new hospital in just a few days as China just has (though the finished product is of questionable quality according to some reports). Imagine a global pandemic with a shortage of key inputs, such as masks: even China, the world’s workshop, experienced this recently. In the worst case we would see shortages of masks, and drugs, and beds, and nurses and doctors. Naturally, the public cry for wider and better healthcare would grow the deeper COVID-19 bites. As such, the potential flow-on effects from a worst-case virus scenario may be as socio-economically substantial as the revolutionary European social reforms that followed the end of World War 1.
Conclusion: just a passing fever?
Indeed, having considered “sick-stemic risk” stemming from COVID-19, we also need to consider the following: against a political tailwind blowing towards right-wing populism anyway, as explored in last year’s The Age of Rage; with businesses already rethinking their global strategies in the wake of the US-China trade war; and with a health-scare now seeing voters panic and look for answers, will we see a more pronounced shift towards anti-globalization movements in the wake of the virus?
The prevailing political trend of “national security” will likely also come into play: “How can it be,” populations will ask, “that we have no local production of virus masks, or drugs? Surely we need to keep them for ourselves first! Why are we allowing foreigners in when they might be infected? Let’s prioritize health and not markets!”
Deglobalization will arguably accelerate – and that is before we address the issue of how states will be able to pay for the higher healthcare spending that populations will demand, which does not sit alongside a small-government, free-trade globalization that we have grown accustomed to.
For now we can see that in the short-term there will undoubtedly be far less global travel and much less trade: we already see that. In the long-term it all depends on how COVID-19 plays out.
If it passes quickly, then just as in 2008-09 the key structural lessons on systemic risk of globalization will arguably be ignored in favour of the obvious near-term benefits, while lip-service is paid to the risks in public. However, should COVID-19 spread and linger, meaning that each new journey, each new encounter means a risk of infection with a 1 in 5 chance of serious illness and a 1 in 50 chance of death (based on data so far), then things may change very significantly on many socio-economic fronts. After all, the word “quarantine” emerged from the established practice in Venice of holding visiting sailors off its coast for 40 days to ensure they did not carry any disease.
To repeat, the lessons of COVID-19 are far older than the century-old Spanish flu: complex interconnected systems may produce what look like superior outcomes/returns in the short-term, but they also greatly increase underlying risks that will eventually emerge at far greater cost. These are multiplicative and exponential rather than additive and linear. Markets still aren’t pricing such outcomes, even after the recent equity sell-off.
Let’s conclude with Søren Kierkegaard again: his seminal work was titled “Fear and Trembling”, which seems appropriate enough today looking at COVID-19 vs. Spanish flu. However, he also argues for a leap of faith and states that “Hope is a passion for the possible.” Indeed.
https://ift.tt/399kz5t
from ZeroHedge News https://ift.tt/399kz5t
via IFTTT



0 comments
Post a Comment